
Vitamin D is one of the most talked-about nutrients in plant-based nutrition — and for good reason. Often called the “sunshine vitamin,” it plays a critical role in calcium absorption, bone health, immune function, and mood regulation. The challenge is that very few foods naturally contain vitamin D, and plant-based sources are even more limited. Whether you’re just starting a plant-based diet or have been eating this way for years, understanding how to optimize your vitamin D status is essential.
Here’s what the latest research and seven leading plant-based doctors have to say about getting enough — through sunshine, supplementation, or both.
What Is Vitamin D and Why Does It Matter?
Vitamin D is a fat-soluble hormone that your body produces when your skin is exposed to UVB sunlight. It regulates calcium and phosphorus absorption, supports immune cell function, and influences over 1,000 genes. Beyond bone health, vitamin D is crucial for immune response — research shows that vitamin D receptors are expressed on many immune cells, including B cells, T cells, dendritic cells, and macrophages. This means vitamin D directly shapes your ability to fight off infections and prevent autoimmune conditions. It also supports neurotransmitter synthesis, regulates serotonin production (affecting mood), and plays a role in cardiovascular health through blood pressure regulation.
There are two main forms: D2 (ergocalciferol), found in mushrooms and some fortified foods, and D3 (cholecalciferol), which your skin produces from sunlight. The critical innovation for plant-based eaters is lichen-derived D3, which is identical to cholecalciferol your skin produces from UVB exposure. This vegan D3 is now widely available and registered with the Vegan Society, making it the most effective option for plant-based supplementation.

How Common Is Vitamin D Deficiency?
Vitamin D deficiency is widespread regardless of diet, but plant-based eaters face additional risk. A 2024 study of Spanish vegans, vegetarians, and omnivores found 93.7% prevalence of vitamin D deficiency or insufficiency, with significantly higher rates in vegans. Among vegans specifically, over 80% fell below 30 ng/mL. A 2025 systematic review identified vitamin D as one of the critical deficiencies requiring attention in vegan diets, consistently appearing across populations. A German study of 662 plant-based individuals found that 76% of vegans had insufficient vitamin D, compared to 42% of omnivores.
Globally, the scope is staggering. An estimated 1.4 billion people worldwide have insufficient vitamin D, making it one of the most prevalent nutritional deficiencies on the planet. The World Health Organization recognizes vitamin D insufficiency as a significant public health concern across all populations. Deficiency varies dramatically by latitude — people living above 40°N latitude, which includes most of North America and Europe, experience seasonal vitamin D insufficiency during winter months. Those above 50°N, including Canada, northern Europe, and Scandinavia, may experience 6 months or more of minimal vitamin D production from sun exposure annually.
Seasonal variation is particularly pronounced. In northern climates, vitamin D blood levels typically drop 20-30% from summer to winter due to reduced UVB exposure. This creates a predictable annual cycle where levels peak in late summer and reach their lowest in late winter. People with darker skin tones show greater seasonal variation due to the increased melanin that reduces UVB penetration — this is why supplementation becomes even more critical for Black, Indigenous, and other people of color living at higher latitudes.
The role of melanin and skin tone cannot be overstated. Individuals with dark skin have 3-6 times less efficient vitamin D synthesis from sun exposure compared to those with fair skin. This means that for Black Americans and others with darker skin, a 20-minute summer sun exposure that produces 3,000-5,000 IU in a fair-skinned person may yield only 500-1,000 IU. For this reason, data from research on predominantly light-skinned populations may underestimate true deficiency risk in communities with darker skin tones. These numbers underscore why supplementation matters, particularly for plant-based eaters living in northern latitudes, with limited sun exposure, or with darker skin tones.
What Do Plant-Based Doctors Recommend for Vitamin D?
Seven leading WFPB physicians share a broad consensus: most plant-based eaters should supplement with 2,000 IU of vitamin D daily, with adjustments based on blood testing and sun exposure.
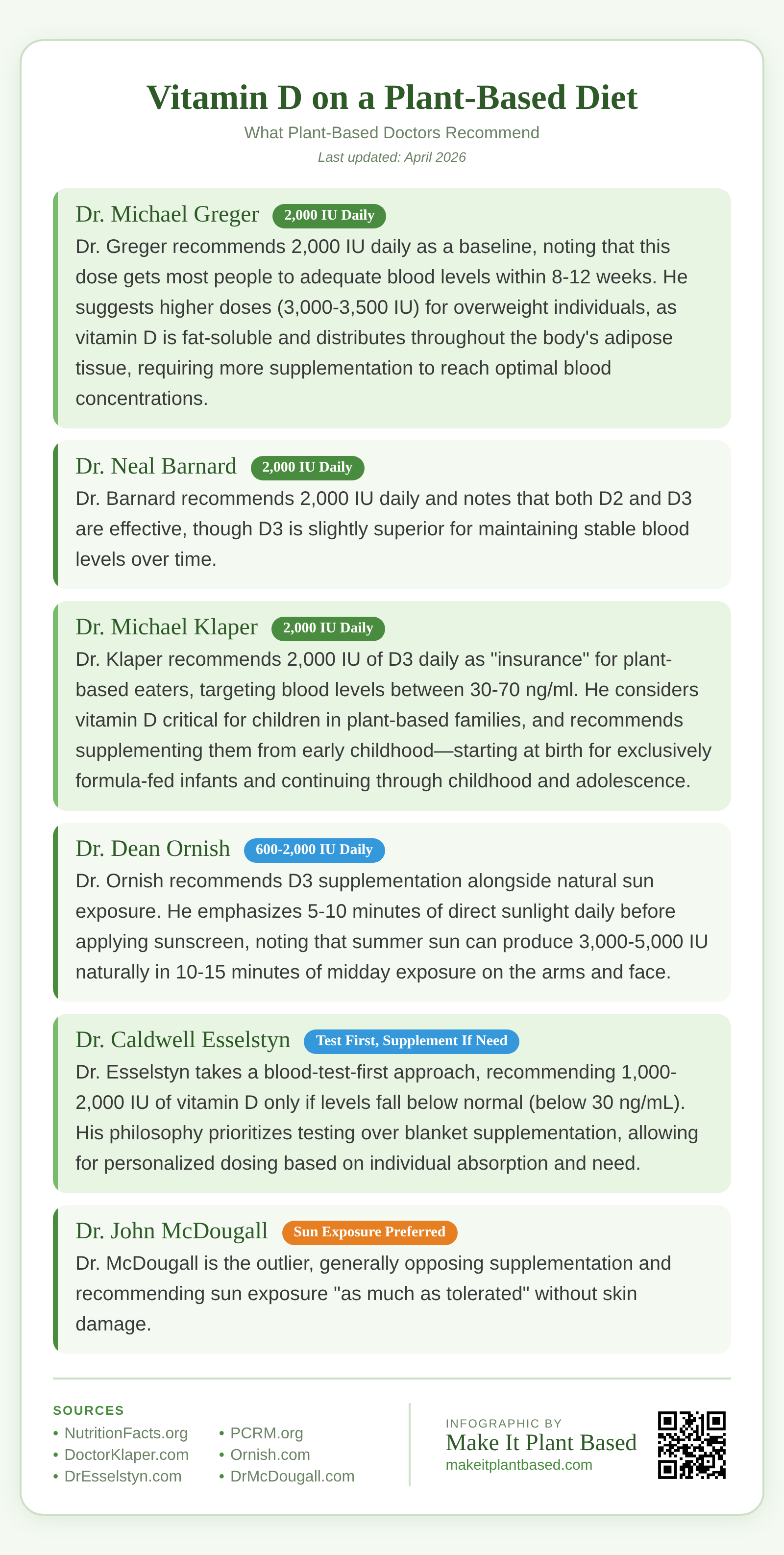
Dr. Michael Greger — 2,000 IU Daily
Dr. Greger recommends 2,000 IU daily as a baseline, noting that this dose gets most people to adequate blood levels within 8-12 weeks. He suggests higher doses (3,000 IU) for overweight individuals, or 3,500 IU for those over age 70, as vitamin D is fat-soluble and distributes throughout the body’s adipose tissue, requiring more supplementation to reach optimal blood concentrations. For those with higher body weight, the vitamin D bioavailability is reduced because the supplement distributes into fat stores rather than remaining in the bloodstream. He emphasizes blood testing to fine-tune dosage and monitor individual absorption variation, as genetics can cause up to three-fold differences in how efficiently people absorb and utilize vitamin D from supplements.
NutritionFacts.org — Vitamin D Supplementation
Dr. Neal Barnard — 2,000 IU Daily
Dr. Barnard recommends 2,000 IU daily and notes that both D2 and D3 are effective, though D3 is slightly superior for maintaining stable blood levels over time. He recommends 20 minutes of sun exposure on the face and arms when possible, with supplementation as backup during low-sunlight months. He emphasizes that winter supplementation is non-negotiable for most temperate latitudes. Through his work at PCRM, Dr. Barnard has observed that plant-based eaters who skip supplementation during winter show average blood level drops of 15-20 ng/mL, whereas those who supplement consistently maintain optimal status year-round. He also notes that sun exposure alone cannot account for individual variation in skin tone, age, and absorption efficiency.
PCRM — What Supplements Do Vegans Need? (Dr. Barnard Q&A)
Dr. Joel Fuhrman — 2,000-3,000 IU Daily
Dr. Fuhrman recommends 2,000 IU daily, increasing to 3,000 IU if blood levels of 25(OH)D fall below 25 ng/ml. He prefers D3 and strongly advocates testing to determine individual needs, as bioavailability varies significantly based on gut health, age, and body composition. Individuals with inflammatory bowel conditions, celiac disease, or reduced stomach acid absorption may require 50-100% higher doses. He recommends testing at minimum annually, ideally both in late winter and late summer to understand your personal seasonal variation pattern. Testing twice yearly also helps identify whether supplementation changes are needed across seasons, and allows for dose optimization before vitamin D becomes critically low in late winter.
DrFuhrman.com — Vitamin D Is Critical
Dr. Michael Klaper — 2,000 IU Daily
Dr. Klaper recommends 2,000 IU of D3 daily as “insurance” for plant-based eaters, targeting blood levels between 30-70 ng/ml. He considers vitamin D critical for children in plant-based families, and recommends supplementing them from early childhood—starting at birth for exclusively formula-fed infants and continuing through childhood and adolescence. He notes that bone development is compromised at low vitamin D levels, with impacts visible even in young childhood through delayed motor development, skeletal deformities, and in severe cases, infantile rickets. Adequate vitamin D during childhood and adolescence establishes peak bone mass, the foundation for lifelong bone health. He emphasizes that children on plant-based diets cannot rely on sun exposure alone, making supplementation non-negotiable.
Dr. Dean Ornish — Sunshine First, Supplement as Needed
The Ornish Lifestyle Medicine program emphasizes natural sun exposure as the primary vitamin D strategy. Dr. Ornish recommends 5-10 minutes of direct sunlight daily on the face and arms before applying sunscreen, as brief midday sun exposure can stimulate significant vitamin D production. His seasonal guidance acknowledges that spring through fall provides the best synthesis opportunity at temperate latitudes, while winter supplementation with D3 becomes necessary when sun exposure is limited. The Ornish program includes vitamin D supplementation as part of its comprehensive approach to cardiovascular reversal, alongside a low-fat plant-based diet, exercise, and stress management. Blood testing is recommended to determine individual needs and guide appropriate dosing.
Ornish.com — Sunshine for Heart Health
Dr. Caldwell Esselstyn — Test First, Supplement If Needed
Dr. Esselstyn takes a blood-test-first approach, recommending 1,000-2,000 IU of vitamin D only if levels fall below normal (below 30 ng/mL). His philosophy prioritizes testing over blanket supplementation, allowing for personalized dosing based on individual absorption and need. He advocates baseline testing before starting any supplementation regimen, then quarterly or biannual testing to assess whether supplementation is achieving target levels. He notes that regular testing prevents both deficiency and excess, and allows for dose adjustments based on real data rather than assumptions. For those whose levels are naturally adequate through sun exposure or other factors, this approach avoids unnecessary supplementation while ensuring those with true deficiency risk receive appropriate treatment.
Dr. John McDougall — Sun Exposure Preferred
Dr. McDougall is the outlier, generally opposing supplementation and recommending sun exposure “as much as tolerated” without skin damage. He considers 20 ng/ml adequate — a lower threshold than his colleagues, though this is below the 30 ng/mL minimum recommended by most endocrinologists for optimal immune and bone health. However, he acknowledges that people living in cloudy climates or with limited outdoor exposure may need supplementation. His position emphasizes that sun exposure, when available, is preferable to supplements. For those with access to consistent sunlight year-round and without risk factors like darker skin tone or advanced age, his approach may be viable, but it remains at odds with the consensus of most plant-based physicians who recommend supplementation as a reliable baseline for nearly all plant-based eaters in temperate climates.
DrMcDougall.com — Vitamin D Values
Sun Exposure vs. Supplements: What Works Best?
Your skin can produce 10,000-20,000 IU of vitamin D from 20-30 minutes of full-body midday sun exposure. However, this depends heavily on latitude, season, skin tone, age, and sunscreen use. People living above 37°N latitude (roughly the line from San Francisco to Richmond, Virginia) cannot produce meaningful vitamin D from sun exposure during winter months — this includes most of the US, Canada, and Europe from October through March.
The sun angle, or zenith angle, is the critical factor. During winter at northern latitudes, the sun never rises high enough in the sky for its rays to pass through the ozone layer at the angle required for UVB penetration to skin. At 52°N latitude (Canada, northern Europe), this vitamin D winter extends up to 6 months annually. The angle of the sun matters even during summer — early morning and late afternoon sun, even at temperate latitudes, are dominated by UVA rays, which do not trigger vitamin D synthesis. Only midday sun (10 AM to 3 PM) at the right angle provides sufficient UVB for reliable production.
Darker skin tones require 3-5 times longer exposure for the same production due to higher melanin content, which reflects and absorbs UVB radiation before it can stimulate vitamin D synthesis. This means that a fair-skinned person in Los Angeles might produce adequate vitamin D from summer sun exposure, while a person with darker skin in the same location may still require supplementation. Sunscreen with SPF 30 reduces vitamin D synthesis by over 95%. And as you age, your skin becomes less efficient at producing vitamin D — people over 60 produce about 50% less vitamin D than younger adults from the same sun exposure, and people over 70 produce less than 25% as much.
For all these reasons, supplementation provides a reliable baseline regardless of your circumstances. Sun exposure remains a valuable bonus when available, but cannot replace supplementation for reliable, year-round vitamin D status in northern climates, for people with darker skin tones, for older adults, or for anyone unable to commit to consistent midday outdoor time.
Signs You May Be Low in Vitamin D
Common symptoms include persistent fatigue that doesn’t improve with sleep, bone or back pain, frequent colds and infections, slow wound healing, muscle weakness, and mood changes including seasonal depression. Many people attribute these to stress or aging without considering vitamin D status.
Bone pain and muscle weakness occur because vitamin D is essential for calcium absorption. Without adequate vitamin D, calcium cannot be properly absorbed in the intestines, forcing your body to pull calcium from bones to maintain blood calcium levels. This leads to weak, aching bones and a mineral density decline visible on DEXA scans. Muscle weakness arises through direct action on muscle cells, which express vitamin D receptors; low vitamin D impairs muscle protein synthesis and ATP production in mitochondria, reducing strength and endurance.
Fatigue has multiple mechanisms. Vitamin D receptors are found in mitochondria, the energy powerhouses of cells. Low vitamin D reduces mitochondrial ATP production, causing pervasive cellular energy depletion. Additionally, vitamin D influences dopamine and serotonin synthesis; deficiency impairs these neurotransmitters, contributing to both fatigue and depression. Seasonal affective disorder is partly driven by reduced sunlight and subsequent vitamin D insufficiency.
Impaired wound healing results from vitamin D’s role in immune cell differentiation and antimicrobial peptide production. Vitamin D receptor expression on keratinocytes (skin cells) and macrophages is critical for skin barrier repair and infection prevention. Studies show that vitamin D-deficient individuals have slower wound closure and higher infection rates in surgical wounds.
Severe deficiency can lead to bone softening (osteomalacia in adults, rickets in children) and increased fracture risk. A review in the Journal of Investigative Medicine confirmed that vitamin D deficiency is associated with increased autoimmunity and susceptibility to infection, as the vitamin D receptor is expressed on immune cells including B cells, T cells, and antigen-presenting cells. A landmark study found that supplementation improves muscle strength and reduces both fall risk and fracture incidence. A simple blood test for 25(OH)D levels can confirm your status — optimal is generally considered 30-50 ng/ml.
Vitamin D Testing and Optimal Levels
A 25(OH)D blood test (the marker doctors use) costs $30-50 and gives you a clear picture of your current status. The results are interpreted as follows: below 20 ng/mL is considered deficiency, 20-29 ng/mL is insufficiency, 30-50 ng/mL is optimal for most people, and above 100 ng/mL may indicate excess (though toxicity typically occurs at sustained levels above 150 ng/mL).
Most plant-based doctors recommend testing at minimum once yearly, ideally in late winter when levels are at their lowest due to reduced sun exposure. If you live in a northern climate or have limited sun exposure year-round, testing twice annually (winter and summer) provides better tracking. After beginning supplementation, retest after 8-12 weeks to assess absorption and adjust dose if needed. Factors affecting absorption include gut health, age, body weight, and genetic variation in vitamin D metabolism — some people require double the dose to reach optimal levels.
For women, testing before pregnancy is valuable as adequate vitamin D supports fetal bone development. Pregnant and nursing women should maintain levels of 30-40 ng/mL minimum. Children should also maintain at least 30 ng/mL for proper bone development and immune function.

Sun Exposure Guidelines: Latitude, Skin Tone, and Timing
The ability to produce vitamin D from sunlight is highly dependent on geographic location and time of day. The relationship between latitude and vitamin D production is governed by the Zenith angle — the angle between the sun’s rays and the vertical line at your location. Across the United States, people above 37°N latitude — including virtually all of the northern half of the country — experience a “vitamin D winter” from November through February where sun angles are too low to produce meaningful synthesis. Those above 52°N (Canada, northern Europe) experience even longer periods of insufficient production, sometimes 5-6 months with inadequate UVB for vitamin D synthesis.
Skin tone significantly affects synthesis rates. Individuals with darker skin require 3-6 times longer sun exposure to produce the same vitamin D as those with fair skin, due to higher melanin concentrations. This means that for Black Americans, supplementation becomes particularly critical during winter months, and may be needed year-round in northern latitudes. Age is another factor — people over 70 produce less than 25% of the vitamin D that younger adults produce from identical sun exposure.
Time of day matters significantly. Midday sun (10 AM – 3 PM) contains the highest proportion of UVB rays. Early morning and late afternoon sun are largely UVA, which doesn’t stimulate vitamin D production. Aim for 10-20 minutes of midday sun exposure on arms and face several times weekly during spring through fall, but understand that this supplementary exposure is just that — supplementary. Supplementation remains necessary for reliable, year-round status.

How to Get Enough Vitamin D on a Plant-Based Diet
Supplementation: Most doctors recommend 2,000 IU of vitamin D3 daily. Look for lichen-derived D3 supplements, which are fully vegan and bioidentical to the D3 your skin produces. Take with a meal containing some fat for better absorption — the vitamin D dissolves in fat and is absorbed more efficiently in the small intestine when dietary fat is present. D3 supplements taken with a meal containing 5-10 grams of fat show significantly better absorption than those taken alone.
Sun exposure: Aim for 10-20 minutes of midday sun on your arms and face several times a week, without sunscreen. This is most effective between April and October at temperate latitudes. Sun exposure alone is unreliable in winter or northern climates, and should never be considered sufficient to meet your needs without supplementation.
Fortified foods: Many plant milks, orange juices, cereals, and tofu are fortified with vitamin D. Check labels — fortification levels vary widely between brands, typically ranging from 100-200 IU per serving. These are useful additions but shouldn’t be relied on as your sole source. UV-exposed mushrooms can also provide meaningful D2, though amounts vary. Place sliced mushrooms gill-side up in direct sunlight for 30-60 minutes to increase D2 content to several hundred IU per serving.
Test your levels: A 25(OH)D blood test costs $30-50 and gives you a clear picture. Test in late winter (when levels are lowest) and adjust supplementation accordingly. Many plant-based doctors recommend testing annually, or twice yearly if you live in a northern climate. After starting supplementation, retest after 8-12 weeks to assess whether your dose is effective.
Vitamin D2 vs. D3: Does It Matter?
The two forms of vitamin D differ significantly in chemical structure and biological potency. D2 (ergocalciferol) is derived from plants and fungi, while D3 (cholecalciferol) is synthesized by animal skin from UVB exposure or produced from cholesterol precursors in animal tissues. Your skin produces D3 specifically, not D2, making D3 the natural form for humans.
D3 is generally considered more effective at raising and maintaining blood levels than D2, particularly at higher doses. Research shows D3 is approximately 87% more potent at raising serum 25(OH)D than D2 at the same dose, and produces 2-3x greater storage of the vitamin in body tissues. This means that equivalent doses of D2 and D3 do not produce equivalent blood levels — you may need significantly more D2 to achieve the same result as a smaller D3 dose. Studies also show D2 has a shorter duration in the bloodstream, with faster metabolism and clearance compared to D3’s longer half-life, leading to more fluctuating blood levels across the supplementation cycle.
D2 was historically the only vegan option (sourced from UV-irradiated mushrooms or yeast), but lichen-derived D3 has changed the landscape entirely. Lichen-derived D3 is now widely available, registered with the Vegan Society, and chemically identical to the D3 your skin produces from sunlight. Most plant-based doctors who specify a preference recommend D3 for this reason — it matches your body’s natural form, produces superior blood level elevation, and maintains more stable levels throughout the supplementation cycle. Lichen D3 has become the gold standard for vegan supplementation.
One exception worth noting: UV-exposed mushrooms can provide meaningful vitamin D2. Placing sliced mushrooms gill-side up in direct sunlight for 30-60 minutes can increase their vitamin D2 content to several hundred IU per serving — a useful dietary boost, though not a substitute for supplementation. If D2 is your only option, research shows doses of 2,000-4,000 IU are needed to match the efficacy of 2,000 IU of D3.
Frequently Asked Questions
How much vitamin D should a vegan take daily?
Most plant-based doctors recommend 2,000 IU of vitamin D3 daily as a baseline. Individual needs vary based on sun exposure, skin tone, latitude, age, and body weight. Blood testing for 25(OH)D is the most reliable way to determine your optimal dose. Those with darker skin, living in northern climates, or over age 60 typically require higher doses.
Can you get enough vitamin D from food alone on a plant-based diet?
It’s very difficult. Few plant foods naturally contain vitamin D, and fortified foods typically provide only 100-200 IU per serving. You would need 10-20 servings of fortified plant milk daily to reach 2,000 IU — supplementation is far more practical. Sunlight exposure can help, but is unreliable in winter or at higher latitudes.
Is vegan vitamin D3 as effective as animal-derived D3?
Yes. Lichen-derived D3 is chemically identical to animal-sourced D3 and raises blood levels equally. It is the preferred form recommended by most plant-based physicians and is officially recognized as vegan.
Can you take too much vitamin D?
Toxicity is rare but possible at sustained doses above 10,000 IU daily without medical supervision. The safe upper limit is generally considered 4,000 IU daily. Blood testing prevents overdosing — aim for 30-50 ng/ml of 25(OH)D. Toxicity symptoms include nausea, weakness, and excessive thirst, but these are uncommon with supplementation.
Take the guesswork out of plant-based nutrition.
Explore our evidence-based guides on the nutrients that matter most.
Browse All Nutrient Guides